Tingling in Hand
Why It Happens and What You Can Do About It
Tingling, numbness, or the sensation of the hand “falling asleep” is a common complaint. This can affect part of the hand, the whole hand, or even just a single finger. In many cases, both hands may be involved.
What Causes Tingling in the Hand?
Tingling usually occurs due to a pinched or compressed nerve. Common sites of nerve compression include:
- Wrist
- Forearm
- Innder side of the elbow
- Upper and outer forearm
- Behind the collarbone (clacicle)
- Neck
There are also medical conditions like thyroid disorders or vitamin deficiencies that can contribute.It may be side effect of certain common medicines including anti hypertensive medicines and antibiotics.
Carpal Tunnel Syndrome (CTS)
This is one of the most common causes of tingling and numbness in the hand. In CTS, the median nerve is compressed at the wrist as the nerve traverses a narrow tunnel.
Symptoms include:
- Tingling or numbness in the thumb, index, and middle fingers, sometimes all fingers.
- More common in females.
- Both hands may be affected.
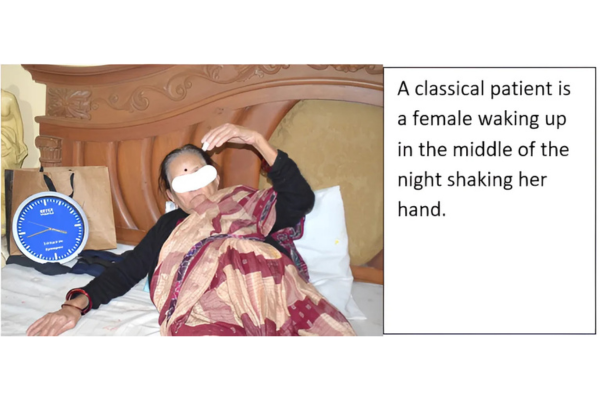
- Symptoms often worsen at night, waking patients up with a need to shake or jerk the hand.
- Dropping objects or difficulty holding a phone or gripping tools.
- Long-standing compression can cause muscle wasting over the thumb, making movements awkward (sometimes misinterpreted as writer’s cramp or dystonia).
- Occasionally, patients report shoulder pain, and only on questioning do they mention hand symptoms.
It’s common to find cervical spondylosis on neck X-rays. However, this is often an incidental finding and not the actual cause of symptoms in most CTS patients.
How Is It Diagnosed?
Your hand surgeon will perform a few simple, painless clinical tests, such as:
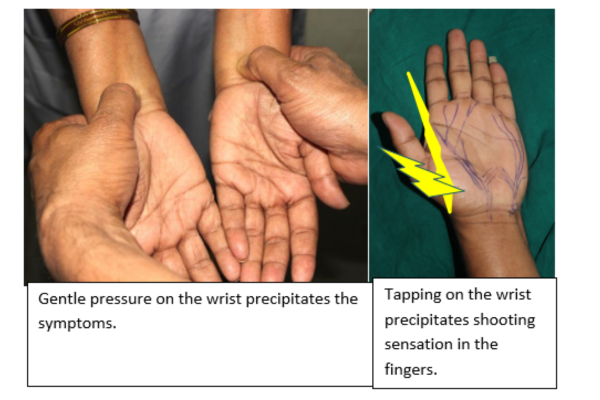
- Phalen’s Test
- Tinel’s Sign
- Reverse Phalen Test
- Durkan’s Test
These tests help identify and confirm Carpal Tunnel Syndrome. To supplement the clinical exam, the doctor might recommend:
- Blood tests (to check thyroid function, vitamin levels, etc.).More tests may be required in selected patients.
- Nerve conduction studies / Electrophysiological tests.
- Ultrasound (USG)of the median nerve to assess swelling in the median nerve.
At times, despite normal test results, a diagnosis can be confidently made on the basis of clinical symptoms alone.
If a neck-originating problem is suspected, an MRI of the cervical spine might be advised, though this is not routinely needed.
Treatment Options for Carpal Tunnel Syndrome
- Wrist Support Splint
Initially, symptoms can often be managed using a cock-up splint, worn:
- At night,
- During periods of rest in the day time.
- The splint is worn for about 4 weeks.
It can be taken off during work or daytime activities. The splint helps relieve pressure on the median nerve.
- Steroid Injection
If the splint doesn’t provide sufficient relief, a single steroid injection together with a numbing solution at the wrist can be very effective and is safe when administered properly. If symptoms resolve even temporarily, it strongly supports the diagnosis of CTS.
- Surgical Release
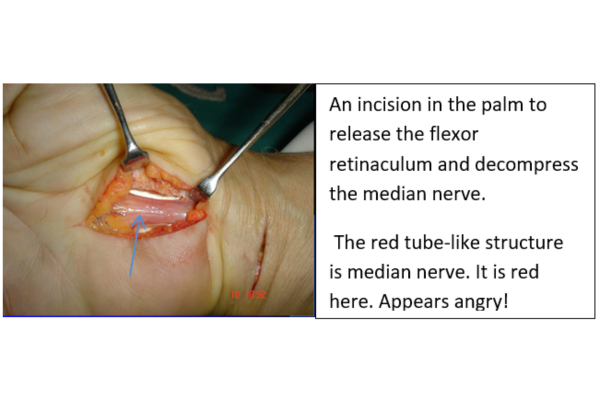
For symptoms that persist despite conservative treatment, a short surgical procedure is recommended. This involves incising the flexor retinaculum to release pressure on the nerve.
- Can be done as a day-care procedure without hospitalization.
- Does not require general anesthesia.
- Involves just a few stitches.
- The wound typically heals in a few weeks.
- Most people can return to work within days.
Both open and endoscopic (keyhole) methods are available. The end results are similar; choice of technique depends on the surgeon’s preference and is always discussed with the patient. Open surgery offers several distinct advantages.Synovium which lines the tendon and is abnormally in excess , can be trimmed making finger excursion easier and better.
The surgical release may be an open surgery as shown or with an endoscope or often referred as a closed surgery . The picture above is considered a gold standard. The wound heals nicely in a few weeks without leaving any scar .
Can symptoms recur after the surgery for carpal tunnel syndrome?
In a very few patients the symptoms can recur. A few treatment options exist for these patients as well.These include repeat examination for additional source of symptoms, wrapping the nerve to prevent scarring of the nerve, Hypothenar fat pad flap. As this is an extensive subject , it is best discussed with the surgeon.
Ulnar nerve compression.
The patient gets tingling in ring and small finger usually while indulging in activities involving prolonged elbow bending,like computer operation or driving a vehicle.There may be weakness of the hand, clawing of the small finger and the ring finger. In more severe affection , the muscles adjacent to the thumb may be wasted.
Examination: The hand surgeon will examine you. One of the tests require, gently tapping the inner side of the arm (Tinel’s Sign) and the elbow which may precipitate tingling along the forearm and the small finger.Other specific test is passively bending the elbow and keeping it bent for a minute . This position may precipitate tingling and numbness.
A few tests may be sought to confirm the diagnosis. These are electrophysiological test/nerve conduction study and ultrasonography(USG) of the nerve .
The ulnar nerve may be affected due to excessive nerve stretching following previous elbow fracture which results in increased angulation of the elbow(Cubitus Valgus).
The ulnar nerve may be affected due to presence of a lump in its course.
Treatment
Avoiding activities where the elbow is kept bent for a long time, helps. If the symptoms persist, this may require surgery. The nerve is known to be compressed at 5 sites on the inner side of the elbow and the upper forearm. There are several surgical options available. The common factor in all the surgical options is to free the nerve from all constricting structures in the region of the elbow. An option shown here is releasing the nerve from its location and anterior transposition of the nerve over the length. The nerve may be decompressed on the inner side of the forearm and the elbow without transposition. This is called decompression in situ. Medial epicondylectomy is another surgical option.
At times, the symptoms persist and needs further evaluation for associated additional compression at additional locations.

Pronator Syndrome
While both conditions involve compression of the median nerve, the compression occurs at different locations. In Carpal Tunnel Syndrome, the nerve is compressed at the wrist, while in Pronator Syndrome, it’s compressed in the forearm, often by the pronator teres muscle or the arch of Flexor Digitorum Superficialis . Pronator Syndrome also causes forearm pain and alters the sensation in the palm, which is always preserved in Carpal Tunnel Syndrome.
Repetitive motions like forearm twisting (pronation), heavy lifting, or activities involving prolonged gripping can lead to irritation or compression of the median nerve in the forearm.
People whose jobs or hobbies involve repetitive use of the forearm—such as athletes, mechanics, factory workers, or those using hand tools regularly—are more prone to develop this condition.
Most cases are diagnosed clinically through a detailed physical examination and specific tests. Imaging like MRI or nerve conduction studies may be recommended if the diagnosis is unclear or to rule out other causes.
In some mild cases, symptoms may improve with rest, activity modification, and anti-inflammatory treatment. However, persistent or worsening symptoms may require physical therapy or surgical intervention.
Most patients recover well after surgery. They can typically resume light activities within a few days and return to full function within a few weeks, depending on the severity and individual healing response.
Radial Tunnel Syndrome
A common cause of upper Forearm Pain is confused with tennis elbow pain.
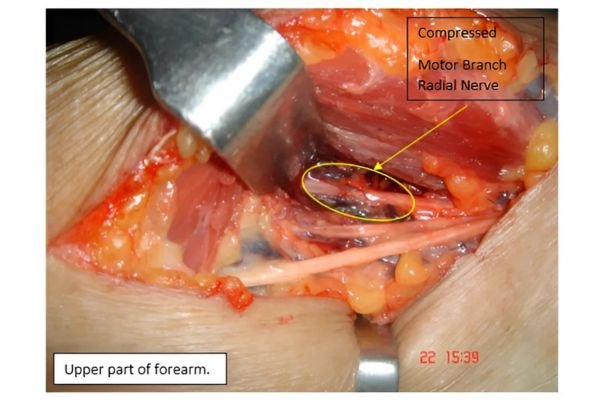
Radial Tunnel Syndrome occurs when the radial nerve, specifically its motor branch called the posterior interosseus nerve, is compressed in the upper part of the forearm. This compression typically happens as the nerve passes under the edge of the supinator muscle, which is thickened and is called the Arcade of Frohse, which is a fibrous arch.
Symptoms
Unlike many nerve conditions that cause tingling or numbness, Radial Tunnel Syndrome affects only motor function. There is no alteration in the sensation. This is because the part of the radial nerve involved is purely motor.
Patients may experience:
- Dull, aching pain in the upper forearm
- Pain radiating toward the elbow or shoulder
- Very rarely there is weakness in wrist or finger extension.
- Discomfort worsens with forearm activity or resisted supination (turning the palm upward)
Notably, there is no tingling or numbness in the hand, which helps distinguish this condition from others like radial nerve entrapment at the wrist or cervical pathology.
Diagnosis
The diagnosis is largely clinical, based on:
- A thorough physical examination. The clinching evidence is the location of the pain which is in the upper part of the forearm over the muscle close to the elbow crease.
- Provocative tests like resisted middle finger active extension and resisted supination
- Careful assessment to rule out other conditions like tennis elbow, cervical radiculopathy.
- Often mistaken for tennis elbow as the location of pain is adjacent. While the pain of tennis elbow is on the bone, the pain in the case of Radial tunnel syndrome is about three finger breaths distally in the muscle.
Ultrasonography may help in the diagnosis.
In some cases, MRI or nerve conduction studies may be used to support the diagnosis or exclude other causes.

Treatment Options for Radial Tunnel Syndrome
- Activity Modification and Rest.Avoiding aggravating movements and allowing the forearm to rest is the first step in management.
- Medications.Short-term use of non-steroidal anti-inflammatory drugs (NSAIDs) can help reduce inflammation and discomfort. One must avoid consuming pain killers for a prolonged period
- Physiotherapy.Gentle stretching and strengthening exercises can help relieve pressure and improve muscle function.
- Surgery (If Needed).If conservative treatments fail, a surgical decompression may be necessary. This involves releasing the structures in the upper part of the forearm compressing the nerve, usually at the Arcade of Frohse. Surgery is typically straightforward and has a good success rate when the diagnosis is accurate .
Thoracic Outlet Syndrome (TOS)
A Condition of Nerve and Blood Vessel Compression Near the Shoulder close to the rib cage.
Thoracic Outlet Syndrome refers to a group of disorders caused by compression of nerves or blood vessels as they pass through the thoracic outlet—the narrow space between the collarbone (clavicle) and the first rib.
Common Symptoms:
- Tingling, numbness, or weakness in the arm and hand. It is crucial to avoid confusing the diagnosis of carpal tunnel syndrome.
- Pain, tightness, or heaviness in the shoulder, neck, or upper chest.
- Discoloration, coldness, or swelling in the arm (if blood vessels are involved).
TOS may involve the brachial plexus (neurogenic TOS), the subclavian vein (venous TOS), or the subclavian artery (arterial TOS).
Treatment:
The treatment begins with postural correction, physiotherapy, and activity modification. The muscles elevating the shoulder are strengthened. If conservative treatment does not relieve symptoms or if vascular compromise is present, surgical intervention may be advised. This often involves a first rib resection to relieve pressure and restore normal function. The bone can be removed through an invisible scar in the axilla.

Don't Let Hand Tingling or Carpal Tunnel Syndrome Hold You Back!
Schedule Your Appointment!
CALL: +91 98220 31140
Frequently Asked Questions
While it may seem minor, untreated Blue Finger can lead to complications like permanent damage or loss of functionality.
Yes, by avoiding prolonged exposure to cold, managing stress, and seeking timely medical care for hand injuries
Recovery varies depending on the severity and treatment method but typically ranges from a few weeks to a few months.